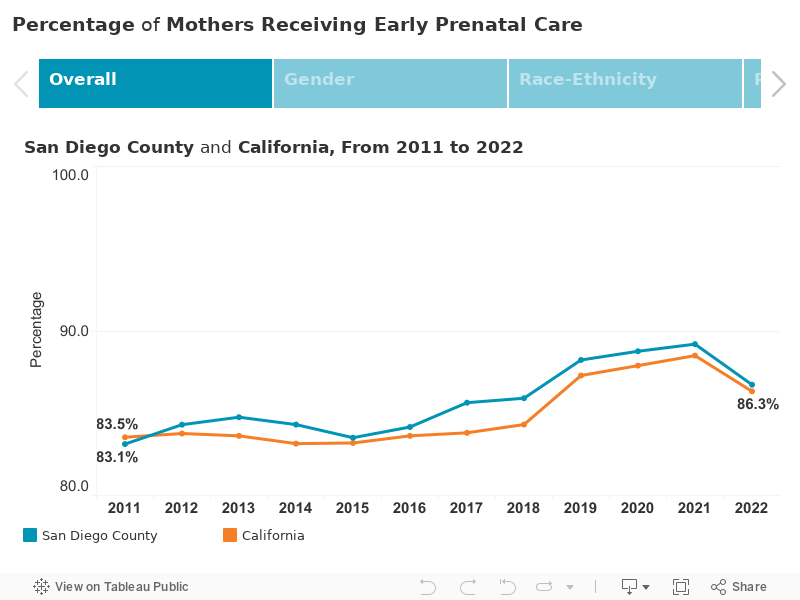
Early Prenatal Care
Infants & Toddlers
Note
*: Statistically unstable
HHSA Regions: Health and Human Services Agency regions
This is a measure of prenatal care initiation and does not account for the frequency of care.
Births with unknown time of prenatal care start are excluded from the total (denominator in rate calculations).
Beginning in 2007, “Date of first prenatal visit” was collected in addition to the “Month prenatal care began” on birth certificates. Therefore, statistics before and after 2007 are not comparable.
Gestation length is based on the obstetric (OB) estimate (last menstrual period (LMP), ultrasound, all perinatal factors). Births with unknown or improbable gestation lengths were classified as unknown (improbable lengths are those that likely reflect inaccuracies rather than actual gestation periods (under 17 complete weeks or 48 or more complete weeks)).
Prior to 2017, for Nativity of Mother, the foreign-born category includes U.S. territories.
The large proportion of births with unknown race/ethnicity affects the accuracy of statistics by race/ethnicity.
Reporting of births that occur in other states/territories is known to be incomplete. From 2017 to 2019, births that occurred outside California are excluded.
California county of residence was determined by geocoding starting in 2022.
Data not available:
Numbers are censored and rates are not calculated when the number of events is fewer than 11. Interpret with caution rates calculated for fewer than 20 events since they are considered statistically unreliable.
Maternal Race-Ethnicity categories:
Hispanic, While, African American/Black, Asian, Native American/Alaskan, Pacific Islander, Two or More Races, Other, Unknown
Source:
State of California, Department of Public Health, Center for Health Statistics and Informatics, Birth Statistical Master Files and California Comprehensive Birth Files.
Prepared by: County of San Diego, Health and Human Services Agency, Public Health Services, Maternal, Child, and Family Health Services (www.sdmcfhs.org), 6/10/2025.
What is the indicator?
This indicator—the percentage of mothers receiving early prenatal care—reflects the proportion of women who receive prenatal care beginning in the first three months (referred to as the first trimester) of pregnancy. These data are recorded on the birth certificate and reported as part of local, state, and federal vital statistics.
Why is this important?
Early and consistent prenatal care reduces the risks of preterm birth, improves birth weight, and promotes healthier infants. Engaging with a qualified healthcare professional is essential for the well-being of both mother and baby. Optimal care involves comprehensive medical services, health promotion, education, psychosocial support, and referrals to nutrition and social services as needed. Preconception care is also recommended to further reduce health risks. Inadequate prenatal care, whether due to late initiation or insufficient visits, increases the likelihood of preterm birth and low birth weight.
What strategies can make a difference?
These evidence-based strategies are used across the country to address early prenatal care:
- Integrated care models, such as patient-centered medical homes and coordinated care teams, provide comprehensive prenatal care addressing medical, social, and psychological needs through combined health education, risk counseling, and medical support.
- Increase outreach efforts to support women under age 20 with enrollment in health coverage and connection with a prenatal provider.
- Expanding prenatal services via telemedicine, mobile clinics, and extended hours helps reach underserved populations. Additionally, transportation assistance and flexible appointment scheduling reduce barriers to care.
- Provide evidence-based, in-person and hybrid-model home visiting programs in the prenatal period, particularly for women with higher medical and social risks.
- Training providers in culturally competent care, motivational interviewing, and effective communication improves prenatal care quality and builds patient trust. Offering culturally and linguistically appropriate services supports this effort.